
Medical Care and Gun Deaths
A common meme claims advances in medical treatments drove gun death rates down.
Like many memes, it fails testing.
Take-aways
- Four major initiatives in emergency treatment have no consistent correlation with gun-homicide/gun-assault ratios
The Claim and Its Problems
With anything political, bad claims can range from irrelevant to irrational. In other cases, it comes from substandard research blindly echoed by activists.
The latter is what we see at the intersection of gun play and medical treatment.
|
We scanned the academic literature and found one specific paper 1 that reported assumed correlations between advancements in medical treatments and a decline in non-suicide gun deaths.
To say the problems with this paper are manifest might be an understatement.
We won’t bore you with all the details, though the table on the right shows some of the deadlier sins therein.
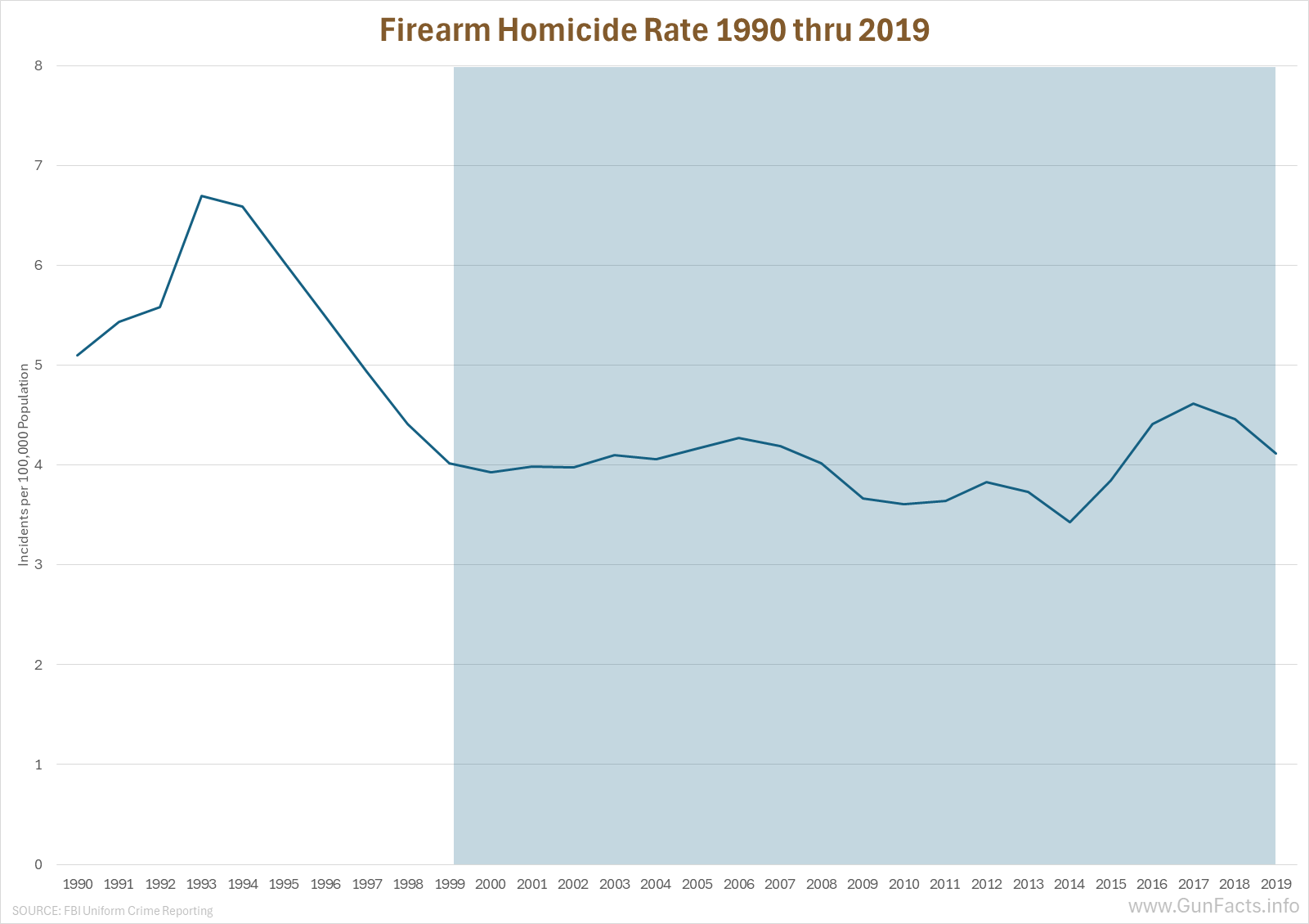
Among the cardinal sins is that much of the study’s timespan includes the massive legislative backlash to the violent crime spiral of the 1980s and early 1990s. Recall that 24 states (including California), with more than half of the country’s population passed habitual offender laws between 1993 and 1996. The study we are rejecting went to 1999. By this time large swaths of bad actors were sent to prison for extended periods of time, including life. Between 1993 and 2003, the state of California alone processed more than 80,000 thugs for second and third strikes.
Nationally, homicide rates plunged.
A Cleaner View
Our acid test study tries to avoid assumptions and irrational proxies.
We look at actual firearm assaults (not all assaults) and non-suicide firearm deaths. We then asked a few AI’s to tally major initiatives to improve medical treatment, both at the emergency medical services (EMS, a.k.a. ambulance or fire-rescue teams) and hospital level, along with the year-range of when the initiative was started and when it was rolled out (sometimes nationally, sometimes only for major metro areas).
Since a firearm assault gets reclassified as a firearm homicide when the victim dies, we used those variables as a more direct measure. The ratio of gun homicides to gun aggravated assaults is a cleaner measure.
 |
 |
 |
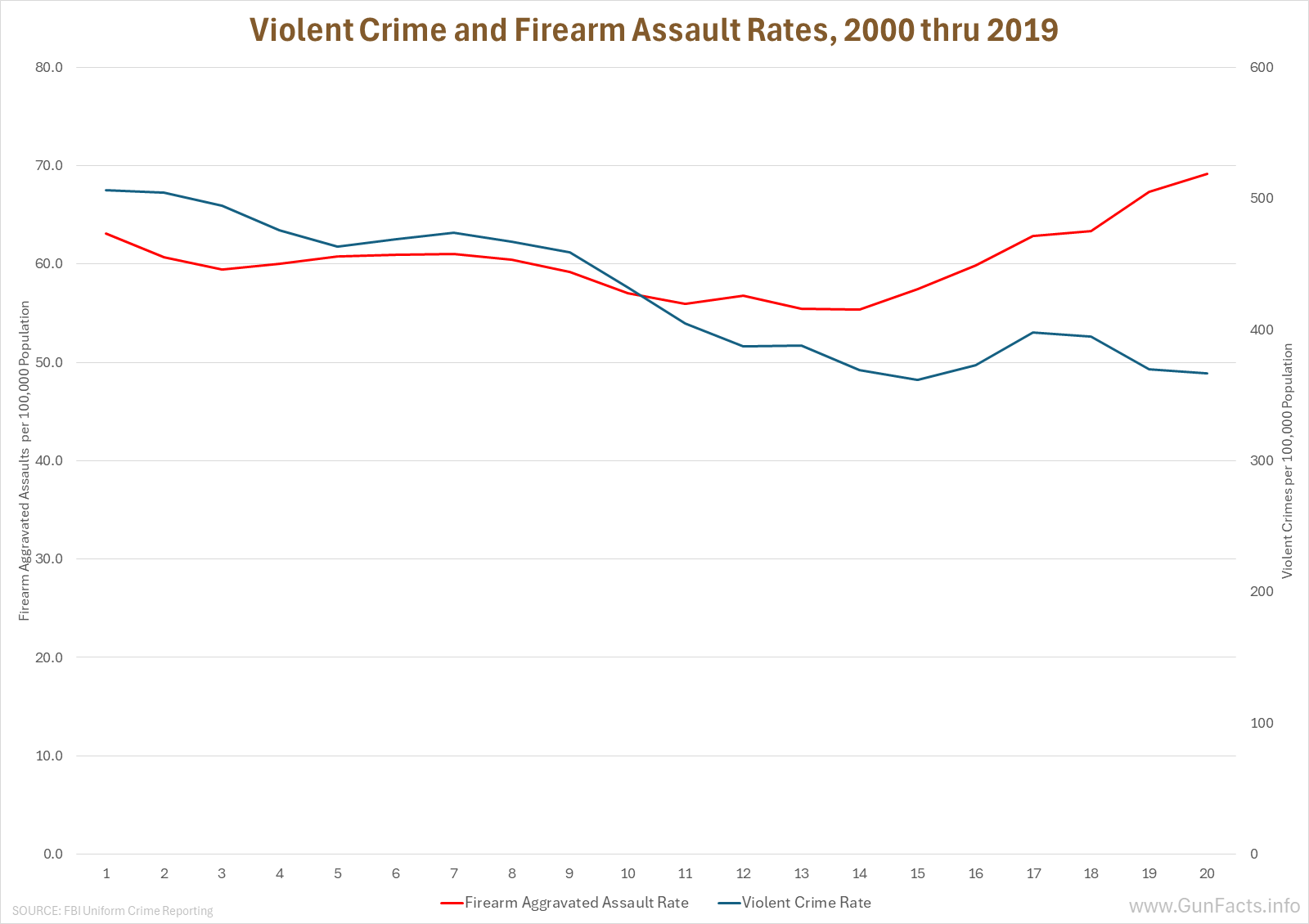
To avoid a bit of confusion later on, we have to note an anomaly in firearm assault rates.
Starting in 2016, the rate of firearm aggravated assaults started rising even as overall violent crime was stable or falling. Troubling as a trend, it also complicates analysis of whether medical treatments lowered gun homicide rates.
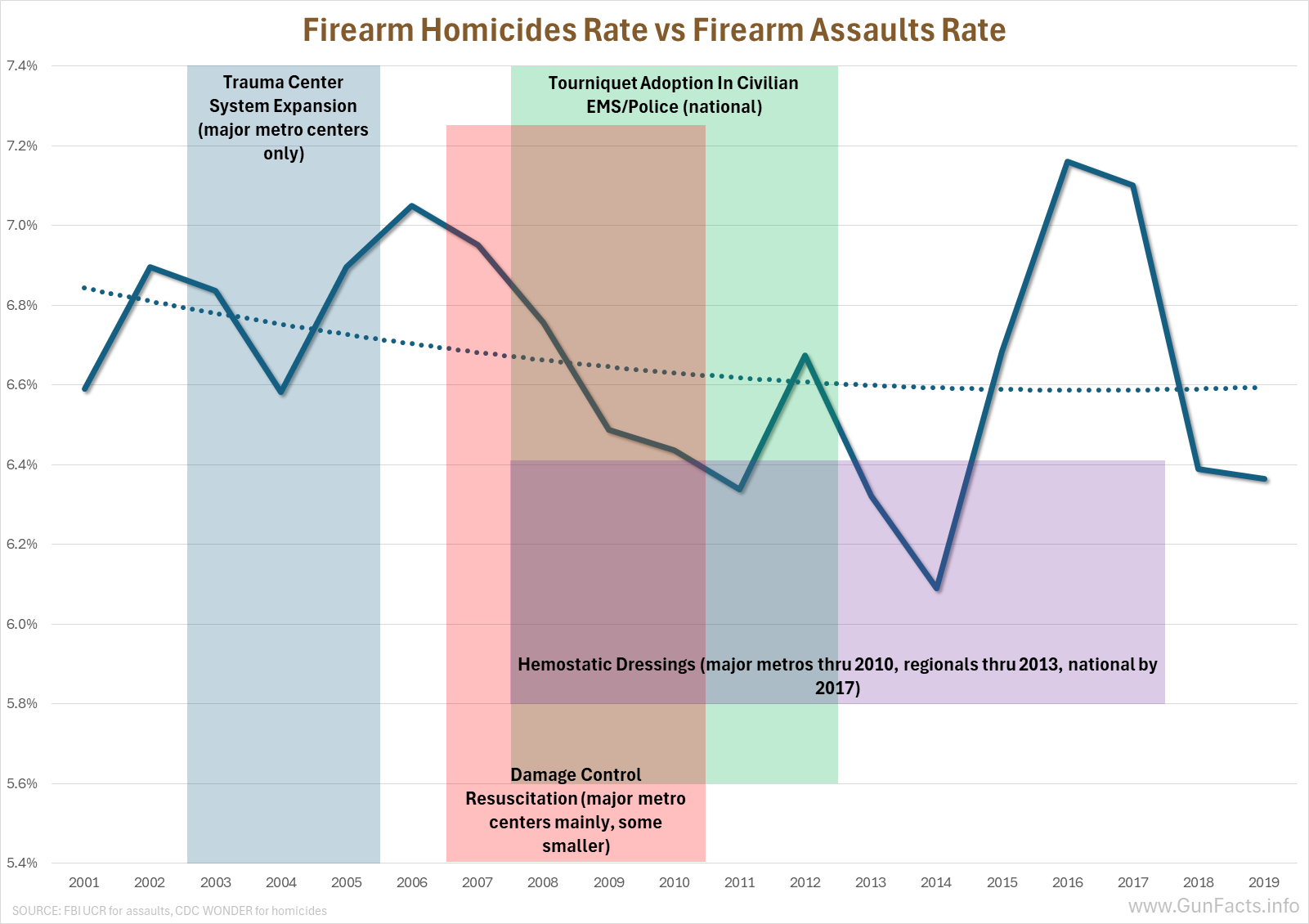
This chart shows the ratio of gun homicides versus gun assaults. We overlayed each of the major initiatives in medical care that would presumably lower the gun homicide rate by keeping a gun assault victim alive.
Here’s the rub: Any new medical protocol or technology would have a “forever after” effect. When you train EMT teams on how to administer tourniquets specifically for gunshot wounds, that benefit does not recede. Any reduction in firearm assault→homicide rate would not reverse (all other things being equal, which they aren’t).
The expansion of trauma centers in the early 21st century, mainly in major metro areas where most street gang gun violence occurs, show an actual increase in the homicide/assault ratio. This is interesting in an of itself. As we exposed in our Top 15 Murder Counties study, gun violence is heavy concentrated in major metro areas, the ones that principally expanded trauma care. Indeed, the majority (53%) of those counties (Cook, Wayne, Saint Louis, Philly, etc.) expanded their trauma care and yet the homicide/assault ratio went up nationally.
Next, we see a short five-year era where two initiatives (tourniquets via EMS and resuscitation in major metros) coincided with a fall in the homicide/assault ratio. One could assume a causal effect, but the rate started dropping in the first year, and returning the homicide/assault ratio to a nominal pre-intervention level in the second year. Other people might argue (though we don’t) that the downward sweep is a byproduct of the 1990s anti-crime push decline.
What happens next is where the “medical intervention lowers gun homicide rates” argument fails the second time. Adding a third intervention (hemostatic dressings) is followed by a sharp increase in the homicide/assault ratio. In other words, after a lull the ratio went up despite three intervention techniques being rolled out, and those followed a general expansion in trauma centers in a majority of overly violent metro areas.
We’ll repeat, because it bears repeating: instutionalized interventions and capacity have no expiration date. The effect (if any) should endure, and the homicide/assault ratio should continue declining as organizational memory and experience adds to the effect. But expanding trauma centers did not reduce the ratio, and the three 2007–2019 interventions saw a spike in the ratio after they were all but fully rolled out.
Do No Harm, but …
Doctors, EMTs, advanced techniques are all good and encouraged. But as a tool for reducing gun deaths from firearm assaults, there is insubstantial evidence they make much—or any—difference.
Notes:
- Murder and Medicine; Harris, Thomas, Fisher, Hirsch; 2002 ↩
It might be interesting to learn how many “gunshot victims” who would otherwise have died before these medical innovations went on to become future “frequent fliers” in the gunshot ward — or to generate others. That would sure have damping effects on the statistics.